
| HOW RADIOACTIVITY CAN AFFECT YOU | Order your RS-500 now! |
Firefighter burned in Chernobyl
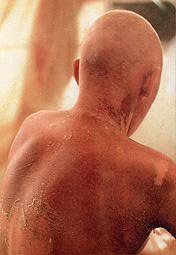 |
Radioactive elements are unstable and give off highly energetic charged particles that can damage the genetic blueprint of the living cell. Some of the time the cell can no longer function or repair itself and dies, but occasionally the cell multiplies uncontrollably and becomes a cancer. Obviously, the size, energy and penetrating distance of nuclear particles determine the damage to living matter and the number of breaks and changes in the genetic code. |
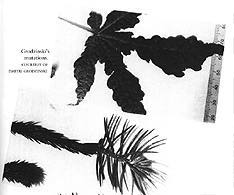
Mutation in leaves after the Chernobyl accident
|
Acute doses can cause a pattern of clearly identifiable symptoms (syndromes). These conditions are referred to in general as Acute Radiation Syndrome. Radiation sickness symptoms are apparent following acute doses > 100 rad. Acute whole body doses of > 450 rad may result in a statistical expectation that 50% of the population exposed will die within 60 days without medical attention. It is generally admitted that an exposure to 300 R during a short period of time (24hr) will be lethal.
A few numbers:
- 600R -- means 100% chance of fatality is expected. Some much earlier - but last within two weeks.
- 400R -- means 50% will die within one to three weeks. Those that don't die are going to be VERY sick and wish that they would. After a few days some may feel better but will often then turn, sicken and die in a few weeks.
- 200R -- lots of sickness, and radiation sickness is pretty terrible (Think of cancer treatment without pain killers.) Lots of vomiting - hair falling out - and all that. Not nice
- 50R -- No fatalities at this level. There is a difference of opinion, as to whether the sickness at this level is physical. Some think, as for example in this very authoritative study, that at this level the sickness is psychosomatic. Whatever its cause it is very general.
- 30R -- Most everyone will feel some sickness - - maybe just "punky" and it may be "just" psychosomatic but it certainly would not be beneficial for children and pregnant mothers. Even this level is a thousand times higher than the maximum general population exposure permitted under peacetime standards.
In the final analysis, fatality is probabilistic, somewhat like car accident fatalities. There have been cases of people getting very much higher radiation and surviving, and others with much lower who have not. Cause and effect become clouded when working with probability issues. There are many impinging factors, such as age, health, medical care, or lack of medical care.
If you are interested in governemnt standards for maximum permissible exposure, please visit our section about risks.
You will find below a study of long-term health effects in the survivors of the atomic bombings of Hiroshima and Nagasaki presented as a list of questions with their answers.
Questions about the Atomic-bomb Survivor Research Program
Reproduced from http://www.rerf.or.jp/eigo/experhp/rerfhome.htm, a Cooperative Japan-United States Research Organization.
The study of long-term health effects in the survivors of the atomic bombings of Hiroshima and Nagasaki
Editor's note: The following questions have been chosen from among many that RERF researchers are often asked. We welcome your questions and comments at research info@rerf.or.jp.
Question 1. How many persons perished in or survived the atomic bombings?
Question 2. How many cancer deaths have occurred among atomic-bomb survivors and how many of these can be attributed to radiation?
Question 3. Because cancer is not always fatal, what is the relationship of radiation to cancer overall?
Question 4. Are radiation-induced cancers still occurring among atomic-bomb survivors?
Question 5. What health effects other than cancer have been seen among the atomic-bomb survivors?
Question 6. What health effects have been seen among persons who were exposed while still in their mothers' wombs?
Question 7. What health effects have been seen among the children born to atomic-bomb survivors?
Question 8. How many atomic-bomb survivors are included in the group being studied by RERF and how were they chosen for this study?
Question 9. What percentage of the original atomic-bomb survivor study population is still alive?
Question 10. How is information about the atomic-bomb survivors obtained?
Question 11. What is meant by "significant" radiation exposure?
Question 12. Are Hiroshima and Nagasaki still radioactive?
Question 1. How many persons perished in or survived the atomic bombings?
Deaths caused by the atomic bombings include those that occurred on the days of the bombings resulting from the collapse of houses caused by the blast and from burns due to heat rays and fires as well as deaths that occurred later from burns and radiation exposure. However, the total number of deaths is not precisely known because records of military personnel in each city were destroyed; entire families perished, leaving no one to report the deaths; and forced laborers were present in unknown numbers. Recent estimates of total deaths occurring within two to four months after the bombings are shown in the Table 1.
Table 1. Estimated population size and number of acute (within two to four months)
deaths in Hiroshima and Nagasaki after the atomic bombings
____________________________________________________________________________
Estimated city population Estimated number of
City at the time of the bombings acute deaths
____________________________________________________________________________
Hiroshima 310,000 persons 90,000-140,000
Nagasaki 250,000 persons 60,000-80,000
____________________________________________________________________________
Five years after the atomic bombings, in the 1950 Japanese national census, approximately 280,000 persons indicated that they "had been exposed" in Hiroshima or Nagasaki. (Although most of them were probably exposed in the former administrative districts of the cities, the census did not require recording the place of exposure.) The census total is a rough estimate of the number of people who were exposed and survived the bombings. References on this subject
 |
Hiroshima and Nagasaki. The Physical, Medical, and Social Effects of the Atomic Bombings. Edited by the Committee for the Compilation of Materials on Damage Caused by the Atomic Bombs in Hiroshima and Nagasaki. English translation by Eisei Ishikawa and David L. Swain, copyright 1981 by Hiroshima City and Nagasaki City. 706 pp. (Originally published in Japanese by Iwanami Shoten Publishers, Tokyo, 1979.) | |
Ohkita T: Annex 4. Health effects on individuals and health services of the Hiroshima and Nagasaki bombs. In Effects of Nuclear War on Health and Health Services, Report of the International Committee of Experts in Medical Sciences and Public Health to Implement Resolution WHA34.38. Geneva, Switzerland: World Health Organization, 1984, pp 101-5. |
|
Medical Effects of the Atomic Bomb in Japan. Edited by A.W. Oughterson and S. Warren. New York: McGraw-Hill, 1956, 477 pp. (This book was based on the 6-volume report of the Joint Commission for the Investigation of the Effects of the Atomic Bomb in Japan. Within a few weeks after the atomic bombings, the Joint Commission, composed of US military and civilian scientists, had been established and was at work in the field. Copies of the original 6-volume report are archived at the US National Academy of Sciences, Washington, DC, and at the RERF Hiroshima Library. |
Return to the list of questions.
Question 2. How many cancer deaths have occurred among atomic-bomb survivors and how many of these can be attributed to radiation?
Analyses of deaths due to cancer among the Life Span Study cohort of atomic-bomb survivors from 1950 through 1990, published in Radiation Research (146:1-27, 1996), are summarized in Table 2. These results are for survivors who were exposed to significant radiation doses (See Question 11).
Table 2. Summary of cancer deaths in the Life Span Study cohort of
atomic-bomb survivors, 1950-1990
___________________________________________________________________________
Estimated number Percentage of deaths
Cause of Total number of deaths due attributable
death of deaths to radiation to radiation
___________________________________________________________________________
Leukemia 176 89 51%
Other types
of cancer* 4,687 339 7%
Total 4,863 428 9%
___________________________________________________________________________
*Solid cancers, such as stomach, lung, breast, colorectal and liver cancers
The number of cancer deaths among the 36,500 Life Span Study survivors who were exposed beyond 2.5 km is 3,177, including 73 leukemia deaths and 3,104 deaths from cancers other than leukemia.The proportion of cancer deaths attributable to radiation exposure is higher among those who were exposed closer to the hypocenter, as in the case of deaths due to injuries from the blast, heat, or radiation. Table 3 presents data on the size of the studied population and the number of cancer deaths in relation to distance from the hypocenter for the approximately 50,000 survivors with significant exposures (See Question 10).
Table 3. Cancer deaths among atomic-bomb survivors, 1950-1990, by distance
from hypocenter
____________________________________________________________________________
Leukemia Other cancers*
_______________________ ________________________
Distance
from Percent Percent
hypocenter No. of No. of attributable No. of attributable
(km) persons deaths to radiation deaths to radiation
_____________________________________________________________________________
<1 810 22 100% 128 42%
1.0-1.5 10,590 79 64% 1156 18%
1.5-2.0 17,370 36 29% 1622 4%
2.0-2.5 21,343 39 4% 1781 0.5%
_____________________________________________________________________________
Because the Life Span Study cohort does not include all survivors (see Question 8), the number of cancer deaths that may be attributed to radiation among all survivors would be larger than the 428 shown in Table 2.
Return to the list of questions.
Question 3. Because cancer is not always fatal, what is the relationship of radiation to cancer overall?
In addition to analyzing cancer mortality (deaths due to cancer), RERF analyzes data on cancer incidence obtained through the cancer registries of Hiroshima and Nagasaki prefectures. Although mortality studies are valuable, the accuracy of cancer diagnoses from death certificates is limited and mortality studies provide little information about the occurrence of cancers with relatively high survival rates. Among 79,972 members of the Life Span Study cohort whose radiation doses were known, 8,613 first primary solid cancers were diagnosed between 1958 and 1987, about three-quarters with histological verification. Significant radiation associations were observed for stomach, colon, lung, breast, ovary, urinary bladder, thyroid, liver, and nonmelanoma skin cancers. Because factors other than radiation can increase the risk of cancer (such as smoking, certain chemicals, various viral and bacterial agents, and so on), RERF researchers are now examining individual types of cancer more carefully to determine what role radiation plays in the mechanism of cancer causation and how it might interact with these other cancer risk factors.
Return to the list of questions.
Question 4. Are radiation-induced cancers still occurring among atomic-bomb survivors?
Yes. The excess risk of leukemia, seen especially among those exposed as children, was highest during the first 10 years after exposure and has continued to decrease throughout the study period. However, the excess risk for cancers other than leukemia continues today, and it seems likely that this excess risk will persist throughout the lifetime of the survivors. About 16% of all cancer deaths and about 25% of the excess--or radiation related--cancer deaths for the period from 1950 through 1990 occurred from 1986 to 1990.
Return to the list of questions.
Question 5. What health effects other than cancer have been seen among the atomic-bomb survivors?
The Life Span Study mortality analyses have revealed a statistically significant relationship between radiation and deaths resulting from causes other than cancer (so-called noncancer diseases). A total of 15,633 noncancer deaths occurred between 1950 and 1990 among the 50,113 persons with significant radiation doses. The overall risk for noncancer deaths is considerably smaller than that for cancer deaths, but because noncancer causes comprise a larger fraction of human deaths overall, the total number of estimated radiation related excess noncancer deaths is about 50-100% the number of estimated radiation related cancer deaths (the reason for the wide range is that the data do not yet clarify the shape of the dose response, and different estimates of number of excess, radiation related, cases result from various shapes of response that can be fit to the data).
Clinical researchers conducting the Adult Health Study of biennial clinical examinations have analyzed the relationship between radiation exposure and a number of selected nonmalignant (non-cancer) disorders. Statistically significant excess risks were detected for uterine myoma, chronic hepatitis and liver cirrhosis, thyroid disease, and cardiovascular disease. The results suggested that the thyroid gland in young persons may be more sensitive to radiation not only in the development of thyroid cancer, but also possibly in the development of nonmalignant thyroid disorders. Although cataracts are another condition related to radiation, their association with radiation seems to be limited to the early years following exposure, as there has been no indication of radiation dose-related excess cases in recent examinations.
Some non-cancer diseases may be associated with altered immune functions in A-bomb survivors. Immunological study of survivors demonstrated that the proportion of helper T cells was significantly decreased with increased radiation dose [see Department of Radiobiology]. Furthermore, the prevalence of myocardial infarction was significantly higher in individuals with a lower proportion of helper T cells. These results suggest that myocardial infarction in A-bomb survivors is partly due to defects of helper T cells. Such defects may contribute towards a reduced immune defense against microbial infections, possibly leading to atherosclerosis.
References on this subject
|
Shimizu Y, Pierce DA, Preston DL, Mabuchi K: Studies of the mortality of atomic bomb survivors. Report 12, Part II. Noncancer mortality: 1950-1990. Radiation Research 152:374-89, 1999 | |
Wong FL, Yamada M, Sasaki H, Kodama K, Akiba S, Shimaoka K, Hosoda Y: Noncancer disease incidence in the atomic bomb survivors: 1958-1986. Radiation Research 135:418-30, 1993 |
Return to the list of questions.
Question 6. What health effects have been found among persons who were exposed before birth?
Among the approximately 3,000 in utero exposed atomic-bomb survivors, the following results have been observed: a reduction in IQ as radiation dose increases, a higher incidence of mental retardation among the heavily exposed, and some impairment in the rate of growth and development on average (not all exposed individuals demonstrated these effects). Many of these effects seem to be particularly pronounced among persons who had been exposed between the 8th and 15th weeks of gestation. Death rates and cancer incidence are being monitored in this group. The numbers of deaths or cancers are still too small to draw any firm conclusions, but the data to date suggest a trend of increasing risk as radiation exposure increases, similar in extent to the trend observed among those exposed to atomic-bomb radiation as children.
Return to the list of questions.
Question 7. What health effects have been seen among the children born to atomic-bomb survivors?
This was one of the earliest concerns in the aftermath of the bombings. Efforts to detect genetic effects were begun in the late 1940s and continue to this day. Thus far, no evidence of genetic effects has been found. Recent advances in molecular biology may make it possible to detect genetic changes at the gene (DNA) level at some time in the future. RERF scientists are working to preserve blood samples that can be used for such studies as suitably powerful techniques are developed (see Repository of biological materials). Monitoring of deaths and cancer incidence in the children of survivors also is continuing.
Return to the list of questions.
Question 8. How many atomic-bomb survivors are included in the group being studied by RERF and how were they chosen for this study?
Current studies of deaths and cancer incidence are based on a sample of 86,500 atomic-bomb survivors who were alive and living in either Hiroshima or Nagasaki at the time of the Japanese national census in October 1950 and for whom radiation dose estimates can be computed. About 50,000 of these persons were exposed to significant radiation doses (Question 11) within a distance of 2.5 km from the hypocenter. The other 36,500 members of the study population were exposed beyond 2.5 km and received very low doses.
In the national census of 1950, approximately 280,000 people indicated that they had been exposed to the atomic bombs. The population studied by RERF probably includes about 50% of the proximally exposed survivors and about 25% of the distally exposed. However, these percentages are not precise because the census did not include recording of the place of exposure.
The cohort includes another group of 27,000 people whose family registry was in one of the cities and who lived in Hiroshima or Nagasaki at the time of the national census but were not exposed to the atomic bomb. However, this latter group is not usually included in analyses because of data suggesting that there are socioeconomic differences from the survivor population. These two groups together are formally known as the Life Span Study (LSS) cohort.
In addition to the Life Span Study, RERF scientists are involved in studies of several other populations. These include the Adult Heath Study (AHS), In Utero Exposed, and Second Generation Cohorts. The AHS population comprises 20,000 members of the LSS, who, since 1958, have been asked to participate in biennial clinic examinations carried out at RERF. About 3,000 people who were exposed to the bombings while in utero make up a second group. Finally, a group of about 80,000 constitute the F1 cohort and include children born to parents with and without exposure to the bombs.
Return to the list of questions.
Question 9. What percentage of the original atomic-bomb survivor study population is still alive?
In 1995, the average age of the surviving atomic-bomb victims was about 66 years. In 1990, about 54% of the RERF study population was still living, and as of 1995, slightly more than 50% were alive. Looking at vital status in terms of age at exposure, we find that at the end of 1990, more than 90% of the survivors exposed under the age of 20 were still living.
Return to the list of questions.
Question 10. How is information about the atomic-bomb survivors obtained?
To make monitoring easier in long-term follow-up of mortality and cancer incidence due to radiation exposure, approximately 90,000 people who were resident in Hiroshima or Nagasaki at the time of the national census on October 1, 1950 were selected from about 280,000 survivors who were directly exposed in Hiroshima City or Nagasaki City.
Information about radiation effects in the atomic bomb survivors is obtained in many ways, some utilizing the full Life Span Study population, others based on subsets of that population. One ongoing method is mortality follow-up, checking for registrations of death and the cause of death. A second ongoing method is checking registrations of cancer diagnoses made by local hospitals and physicians to the cancer registries in Hiroshima and Nagasaki prefectures. Mail surveys asking about lifestyle and other factors have been sent approximately every 10 years to the Life Span Study cohort members. A subset of the Life Span Study (the Adult Health Study) is examined clinically every two years; this clinically examined subset also forms the basis of cytogenetic, immunological, and molecular epidemiologic studies. Chromosome aberrations and blood proteins have been examined in a sample of approximately 8,000 and 24,000 children (respectively) born to one or two radiation exposed parents to assess possible genetic damage passed on to children. Approximately 76,000 children were examined at birth and at age 9 months, between 1948 and 1954, for possible congenital birth defects. Finally, plans are being made to assess the health status of children of atomic-bomb survivors based on mail questionnaires and clinical examinations.
Return to the list of questions.
Question 11. What is meant by "significant" exposure?
In the discussion of cancer risks presented here, attention is focused on survivors with estimated doses greater than 5 millisieverts (mSv; 0.005 Sv). While no excess risks of cancer or other diseases are detectable among survivors with doses at the low end of this range, a dose of 5 mSv is several times higher than the typical annual background radiation level to which people are exposed in daily life (1-2 mSv), or about one-fourth of the currently accepted maximum annual dose allowed for radiation workers (20 mSv). Survivors with doses of 5 mSv or more were typically within about 2.4 km of the hypocenter in Hiroshima and within 2.6 km of the hypocenter in Nagasaki. The average dose received by the group of survivors considered here is about 200 mSv. The radiation dose decreases by about one-half for every 200-meter increase in distance from the hypocenter. (see Dose estimates by distance).
Return to the list of questions.
Question 12. Are Hiroshima and Nagasaki still radioactive?
No. There are two ways radioactivity is produced from an atomic blast. The first is due to fallout of the fission products or the nuclear material itself, ie, uranium or plutonium that contaminate the ground. (Similar ground contamination occurred as a consequence of the Chernobyl accident but on a much larger scale. Click here for more-detailed explanation.) The Hiroshima and Nagasaki bombs exploded at 500 to 600 m of altitude, then formed huge fireballs that rose with ascending air currents. Subsequently, the material cooled down and started to fall with rain. Because of the wind, the rain did not fall directly on the hypocenter but rather in the northwest region (Koi, Takasu area) of Hiroshima and the eastern region (Nishiyama area) of Nagasaki. Nowadays, the radioactivity is so miniscule that it is difficult to distinguish from trace amounts of radioactivity caused by atmospheric atomic-bomb tests.
Another way radioactivity is produced is by neutron irradiation of soil or buildings. (Neutrons comprise 10% or less of A-bomb radiation; nonradioactive materials become radioactive after absorbing neutrons. In contrast, gamma rays--which comprise the majority of A-bomb radiation--do not cause ground materials to become radioactive.) However, most of the radioactivity decayed very quickly so that it now takes months to measure the radioactivity using highly sensitive equipment. Despite miniscule levels, these measurements are currently utilized to estimate neutron doses released from the bombs.
In both cases, the residual radioactivity is far less than the dose received from background radiation; hence, there are no detectable effects on human health.
![]()
Our new RS-500 radioactivity detector and meter measures nuclear radiation levels from the lowest background levels up to 999 mR/hr (10,000.00 µSv/h) (a level that can be reached only in a major nucelar accident or after the explosion of a nuclear weapon). This is 20 times more than ordinary radiation detection devices.
When set on, the alert will beep at a radioactivity level of 1mR/hr (standard nuclear industry radiation alert level).
The RS-500 radioactivity detector detects and measures Alpha, Beta, Gamma and X-Rays (A-B-G-X) radiation. Its digital display is easy to read and does not require switching between scales.
The RS-500 radioactivity detector is as portable as a small cell phone. It is designed for professional and personal use.
Because nuclear emergencies (nucelar terrorist attack, nuclear weapon, radioactive contamination, nukelar accident, etc...) may produce high to very high levels of radiation, the RS-500 high range makes it the best choice for Police departments, security and military personnel, as well as for individual and family safety. Other devices generally saturate before radiation levels become really dangerous and can measure only "safe" radiation levels. They become useless when they are most needed!
We recommend you keep your radiation detector at all time inside the vehicle you would use in case of a radioactivity emergency. This may save precious time should a major radioactive threat occur .